
By: Mary Tassone
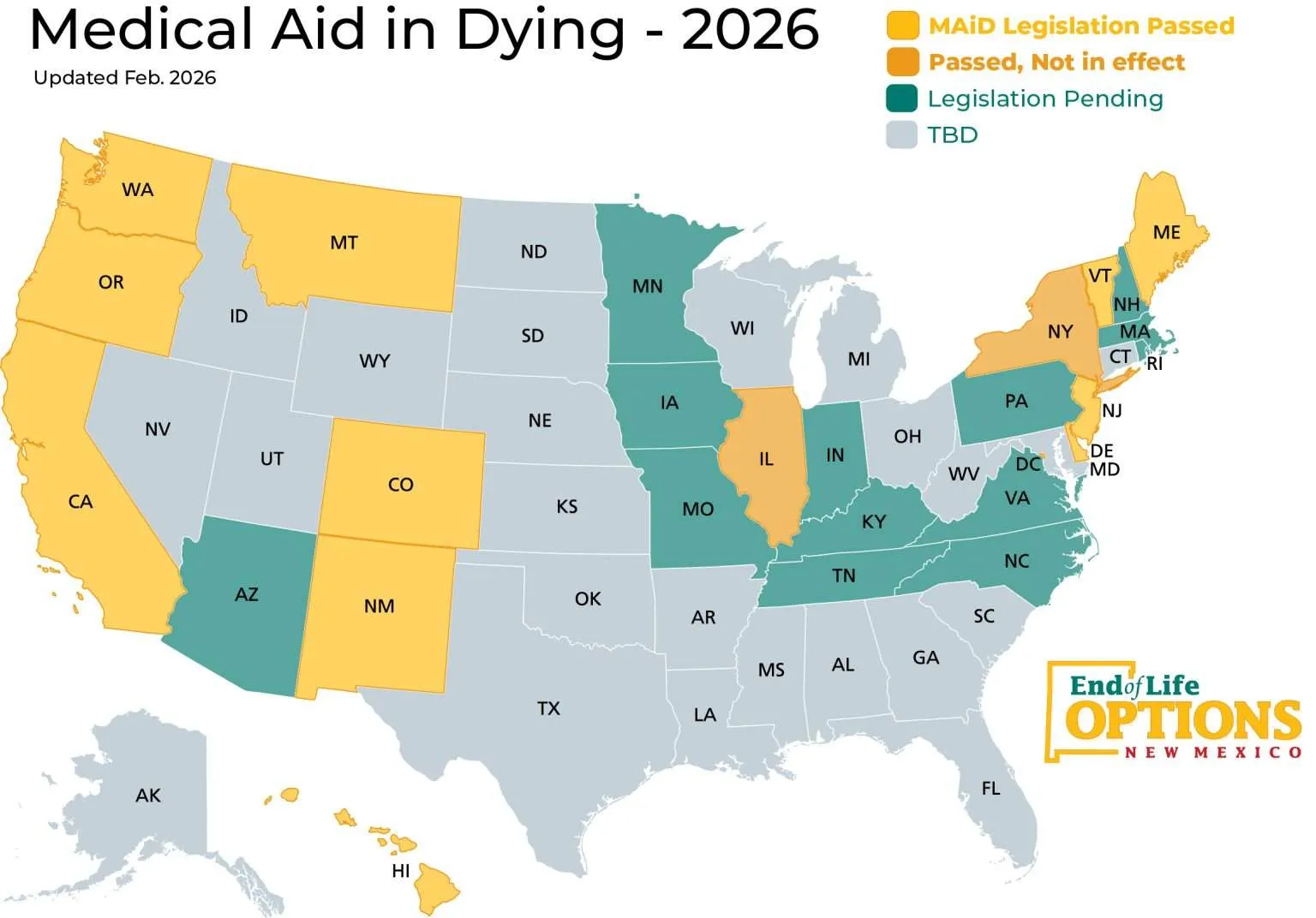
New York has recently signed the Medical Aid in Dying Act (MAiD). [2] MAiD allows mentally competent, terminally ill patients to request medical aid to end their lives under strict procedural safeguards. With the signing of this Act, New York becomes the thirteenth state to authorize MAiD. [3]
This development is a significant shift in state policy. In 2017, the Myers v. Schneiderman decision held in that medical aid in dying falls within the state’s prohibition on assisted suicide as it involves intentionally providing the means to commit suicide. [4] The New York Court of Appeals highlighted the state’s legitimate interest in preserving life, preventing suicide, protecting vulnerable individuals, and maintaining the integrity of the medical profession. [5]
The legislature has turned the state in a different direction. There has been a wide array of ethical and political debates surrounding medical aid in dying. Controversies also arise in the field of science. When science and medication can no longer cure or alleviate pain, should science and medication have a role in ending it?
Not all diseases and illnesses are curable. Advancements in medical technology have extended life and improved the quality of life. However, many cancers remain incurable in advanced states. ALS, a neurodegenerative disease, remains incurable. Science helps diagnose, treat, and manage pain, but it cannot always cure the disease. This raises the idea as to whether science should help end suffering even if it ends life. Is science obligated to prolong life, even if it consists of unavoidable suffering?
The New York MAiD regulates medical intervention to end life. The law signed by Governor Hochul includes strong safeguards to prevent coercion and abuse. In order to be provided with medical aid in dying under the New York Act, a patient must have a diagnosis of 6 months or less to live, a patient must make both recorded oral and written requests for such mediation, and the patient must be deemed to have decision making capacity. [6] The patient’s attending physician must examine the patient in person and patient health records to determine diagnosis and prognosis. [7] The attending physician must also make a determination about the patient’s decision-making capacity and decide that the patient made an informed decision, voluntarily, on their own volition, and without coercion. [8] The attending physician must also refer the patient to a consulting physician and a mental health physician who must corroborate the attending physician’s thoughts. [9] The attending physician must explain the diagnosis, prognosis, risks of the medical aid in dying medication, feasible alternatives, and the ability to rescind the request. [10] They must also give the patient educational information regarding hospice and palliative care. [11] Additionally, if all other requirements are fulfilled, the prescription shall not be fulfilled after the prescription was written for 5 days, creating a mandatory five-day waiting period. [12]
With the rise of do-not-resuscitate orders, withdrawal of support, and palliative sedation, MAiD follows contemporary medicine practices that may not always preserve life at all costs. The New York Medical Aid in Dying Act reflects a shift in how society understands the role of science at the end of life. Science is able to extend life, but MAiD allows science to serve patients’ autonomy and dignity at the end of their life. MAID reflects an intersection between innovation and regulation.
Sources:
[1] Our History, End of Life Options New Mexico, (last accessed March 5, 2026) https://endoflifeoptionsnm.org/about-us/our-history/.
[2]Wendy Hoey Sheinberg, Medical Aid in Dying is Now Legal in NY, Rivkin Radler LLP, February 18, 2026, https://www.rivkinradler.com/publications/medical-aid-in-dying-is-now-legal-in-ny/.
[3]Id.
[4]Myers v. Schneiderman, 85 N.E.3d 57, 62 (2017) (“Aid-in-dying falls squarely within the ordinary meaning of the ordinary meaning of the statutory prohibition on assisting suicide.”).
[5]Id. at 91.
[6]N.Y. Pub. Health Law § 2899-e (McKinney 2026); N.Y. Pub. Health Law § 2899-f (McKinney 2026).
[7] N.Y. Pub Health Law § 2899-f (McKinney 2026) (allowing patients to be seen by the physician via telehealth if the patient would suffer extraordinary hardship, like pain or suffering, if required to meet a physician in-person).
[8]Id.
[9]Id.
[10]Id.
[11]Id.
[12]N.Y. Pub Health Law § 2899-f (McKinney 2026).